The next few months we’ll be highlighting authors who have published in Culture, Medicine, and Psychiatry.
Scott D Stonington, Associate Professor of Anthropology and Internal Medicine, University of Michigan Ann Arbor
Scott Stonington is a cultural anthropologist and internal medicine physician. His first book, The Spirit Ambulance, won awards from multiple academic societies for ethnographic writing. His two major current projects address affect in clinical practice in the U.S. and pain management in Thailand.
In early COVID in the hospital, clinicians were driven into scientific and data-hungry frenzy trying to understand the virus, making their clinical practice very unstable, changing dozens of times daily in response to tweets, texts and news articles. The article is a case study on the dependence of clinical knowledge and practice on context, in contrast to the usual assumption that it is the “view from nowhere.”
Tell us a little bit about yourself and your research interests.
I practice hospital and primary care medicine, which makes me constantly look at social theory and ethnographic concepts through the lens of lived experience. My research always seems to return to that.
What drew you to this project?
I was thrust into working in the hospital in early COVID, at a time when I thought there was a good chance that I would die if I became infected (due to comorbid illnesses). I simply had to study that experience.
What was one of the most interesting findings?
The most interesting finding was that clinicians, afraid and trying to sort through rapid-fire contradictory ideas about COVID, entered a kind of trance, a bad trip, needing to imagine (or “hallucinate”) virus distributed everywhere. It was interesting that the fear wasn’t simply formless emotion, but that it infiltrated the very scientific expertise that they had previously thought of as objective.
What are you reading, listening to, and/or watching right now? (Doesn’t have to be anthropological!)
I just finished Children of Time by Adrian Tchaikovsky. I thought it was just for pleasure, but there were so many wonderful ideas in it that it got my academic idea mill churning!
If there was one takeaway or action point you hope people will get from your work, what would it be?
I think that we fantasize that doctors should be completely objective, and it blinds us to some of the very important effects that their own emotion and experience injects into health systems.
The next few months we’ll be highlighting authors who have published in Culture, Medicine, and Psychiatry.
Senior Research Fellow, University of Queensland
Nathalia Costa is passionate about deepening the understanding of healthcare issues through qualitative methods and methodologies, with a focus on theoretically grounded, critical, reflexive and collaborative approaches. She advocates for pluralist inquiries to achieve the intersubjective understandings needed for impactful collective action.
This critical rapid review examined non-clinical psychosocial support services for culturally and linguistically diverse (CALD) populations delivered by lay health workers. Drawing on a critical realist framework and Brossard and Chandler’s taxonomy on culture and mental health, the review analysed 38 studies (10 quantitative, 7 mixed-methods, and 21 qualitative), mostly conducted in North America and Europe. While many interventions focused on specific populations (e.g., refugees, Latinx immigrants) and targeted outcomes like depression and trauma, fewer studies used multimodal approaches or focused on broad populations. Despite short intervention durations, most reported positive psychosocial outcomes. Qualitative findings underscored barriers such as inadequate resources and limited cultural alignment. The review found most studies operated within split-relativist paradigms, aiming to help participants navigate Eurocentric systems. Culturally responsive and context-sensitive models, prioritisation of social determinants of health and community engagement are likely to be critical to ensure best practice in non-clinical psychosocial support.
Tell us a little bit about yourself and your research interests.
I am a Brazilian scholar living and working in Australia, and committed to shaping, enhancing and transforming quantitative evidence through qualitative methods and methodologies to make research, practice and education more inclusive and nuanced. With postdoctoral studies in policy and at the interface of clinical science and sociology, I draw from these disciplines to explore healthcare challenges and generate insights that drive meaningful change.
What drew you to this project?
I was drawn to this project through my longstanding collaboration with A/Prof Rebecca Olson and Dr Jenny Setchell, with whom I share a commitment to social justice and critical approaches to health research. An opportunity to evaluate a service providing non-clinical psychosocial support for people from multicultural backgrounds came up, and we thought it was important to ground our evaluation in a rigorous and critical understanding of best practice in this area. Rebecca invited me to co-lead the rapid review with her, and I enthusiastically accepted, seeing it as a valuable opportunity to contribute to work that aligns with my values and interests in diversity and policy-informed research.
What are you reading, listening to, and/or watching right now? (Doesn’t have to be anthropological!)
I have been reading The view from Nowhere, by the philosopher Thomas Nigel. It is a book about subjectivity and objectivity – he argues that pure objectivity is impossible because we are embodied, situated beings. As far as I can tell from what I read so far, the book calls for a balance between subjectivity and (inherently limited) objectivity.
If there was one takeaway or action point you hope people will get from your work, what would it be?
It would be great if researchers and practitioners working in non-clinical psychosocial support for people from multicultural backgrounds to move beyond eurocentrism and individualistic understandings and approaches to mental ill-health, and instead adopt approaches that are grounded in an understanding of social, cultural, structural, historical and political contexts.
The next few months we’ll be highlighting authors who have published in Culture, Medicine, and Psychiatry.
Nader Abazari holds a PhD in clinical psychology. Currently, as a post-doctoral researcher, he explores ways to enhance existential well-being through interdisciplinary approaches. He is particularly interested in how cultural context contributes to the fundamental human need to quest for meaning in life.
Existential well-being research group, University of Eastern Finland
Everyone, at some point, faces the question: What makes life worth living? Psychologists address this through the concept of “meaning in life.” As meaning is not automatically given, we must actively create it. While this is a deeply personal process, it is also shaped by the cultural context in which we live. In addition, anthropologists view myths as the essence of the cultures from which they emerge. This led us to ask: Do myths contain clues for meaning-making that remain useful today? To explore this, we compared three psychological theories with examples from world myths. Our analysis shows that mythological narratives, aligned with contemporary theories, provide valuable insights into the meaning-making process: encountering a profoundly impactful event, dissatisfaction with the current state, meaning-making attempts, and providing a vision of desired state. Thus, we conclude that myths remain relevant to enduring human concerns, guiding reflection on meaning in contemporary life.
Tell us a little bit about yourself and your research interests.
Previously, I worked as a psychologist focusing on improving the well-being of individuals with chronic conditions. As a postdoctoral researcher, I found the perfect opportunity to pursue my interest in a particular dimension of well-being, existential well-being. Within this field, I am especially fascinated by sources of meaning, the avenues people draw upon to see their lives as meaningful. These sources range widely, from spirituality, love, and unison with nature to religion, ritual, achievement, freedom and more. What intrigues me most is how people seem to choose their sources of meaning from a kind of “menu” offered by their cultural context. For instance, in Finland, with its striking and abundant natural landscapes, people’s lives are deeply intertwined with nature, and unison with nature often becomes a particularly valued source of meaning. In other countries, however, we may find that sources such as religiosity and spirituality are more prominent. Currently, under the supervision of Associate Professor Suvi-Maria Saarelainen, I am exploring how culture shapes sources of meaning, with myths, as cultural showcases, forming a central part of our research.
What drew you to this project?
In answering this question, I am reminded of Isaac Newton’s famous words: “If I have seen further, it is by standing on the shoulders of giants.” We believe this perspective extends far beyond the academic world; it also applies to everyday life. In the context of meaning in life, these “giants” are the tangible and intangible cultural heritage passed down through generations. Our project was inspired by the idea that just as personal human history can provide insights into how to find meaning in life, collective human history also has the potential to show how our ancestors found meaning in their lives. We sought to take an initial step in showing that the meaning-making practices of the past may still resonate and continue to shape the ways people seek meaning today.
What are you reading, listening to, and/or watching right now? (Doesn’t have to be anthropological!)
Lately, I have been drawn to books that build bridges between human psychological processes, culture, and history. Two that stand out for me are The Cultural Animal by Roy F. Baumeister and The Cry for Myth by Rollo May. I also enjoy podcasts on world history and the biographies of influential figures from diverse fields. For me, history offers a process-oriented, holistic perspective for understanding human issues, and helps me avoid the trap of tunnel vision.
If there was one takeaway or action point you hope people will get from your work, what would it be?
I would say that myths are not just stories of the past, they are lived and culturally validated roadmaps for a meaningful life. They remind us that the visions for a better life that once guided our ancestors can still, at least at times, inspire and shape our own search for meaning today.
The next few months we’ll be highlighting authors who have published in Culture, Medicine, and Psychiatry.
Galia Plotkin-Amrami, Senior Lecturer (Assistant Professor) in the School of Education, University of Ben-Gurion in the Negev, Israel
Galia Plotkin-Amrami’s academic track began with training in anthropology and school counseling and evolved into historical anthropological research on therapeutic discourse during her PhD and several years thereafter. Her more recent research focuses on the medicalization of childhood, parental subjectivity, and stigma in relation to neurodevelopmental disorders and atypical gender performance.
The article focuses on Israeli mothers of children with ADHD. We explored how mothers understand the category of ADHD, their children’s experiences, and their own role over the course of their children’s lives. Our analysis of mothers’ narratives revealed they did not experience the formal diagnosis as an endpoint that settled the understanding of the child’s condition. Rather, they continued to revisit their perceptions of ADHD and their own responsibilities. As an invisible, yet socially disturbing disability, the diagnosis of ADHD does not bring relief from blame. We discuss some features of the Israeli cultural portrait of the child with ADHD that differ from aspects of the ADHD life experience that are emphasized in ethnographies in North American families. We show that emotional vulnerability and risk of social isolation of the child reflect cultural notions of Israeli childhood and shape Israeli mothers’ experiences and decisions related to the child.
Tell us a little bit about yourself and your research interests.
For several years, my main research interest was mental health knowledge and practices in the areas of immigration, trauma treatment, and resilience education. I explored the interrelations between professional knowledge, national ethos, religious narratives, and ethics in the Israeli cultural and political context.
I have begun exploring a different topic—the medicalization of childhood. My recent project focuses on how parents and teachers understand and apply the ADHD category within the school and family context in Israel. In addition, I conduct research with colleges on homeroom teachers’ roles and perceptions of mainstreaming students with emotional-behavioral difficulties within the regular school setting.
Another research project focuses on the parenting of transgender and gender-variant children. It examines how children’s atypical gender performance and gender transition are navigated in the family and school arenas within different educational settings in Israel: Jewish state (secular) schools, Jewish state-religious schools, and independent schools.
What drew you to this project?
The idea of this project emerged from my teaching. My general interest in diagnostic categories and “making up people” led me to teach on the subject. Based on discussions with my students and the understanding that there is no anthropological-historical research in Israel, a highly medicalized society, on medicalization of childhood, I thought it would be appropriate to study the topic. The project focuses on the knowledge and practices of mothers of children with ADHD and teachers who meet such children in the school arena, but I intend to continue to study medicalization, this time by exploring the epistemic culture of the experts involved in diagnosing and treating the disorder among children in Israel. My previous projects on professional discourses in the field of trauma or immigration showed the importance of an anthropological examination of processes of knowledge–generation on mental phenomena. After studying the narratives of mothers and teachers, I see great value in research on medicalization at different levels, macro and micro, institutional and interactive, through the knowledge of formal experts and the expertise of laypeople. Ultimately, the role of mothers or teachers is critical in medicalization processes and, more generally, in the way we understand the concept of disability, norm, and pathology and perceive personal and social responsibility. I hope to continue this research in order to produce additional insights into the uniqueness of the globalized tendency of medicalization in a local context.
What was one of the most interesting findings?
One of the interesting findings for me was the variety of the effects of diagnoses and biomedical explanations on people’s lives and subjectivity and how important it is to pay attention to the narrative, institutional, and moral effects of the diagnosis. For the mothers in our study, the diagnosis of ADHD allowed them to achieve very different goals and was translated into very different decisions, moral experiences, and practices. In addition, we saw the extent to which local perceptions of childhood, well-being, and normative functioning shaped mothers’ decisions to diagnose their children and influenced their interactions with professionals and educators.
What are you reading, listening to, and/or watching right now?
I’ve been listening to a local podcast “On Life and Death.” This podcast is built on an Israeli journalist’s in-depth interviews with people of different ages, mostly writers or those who write, about their experiences of loss at different stages of their lives, their insights around grieving, commemoration, and life, and their moral significance. I began to listen this podcast after a loss in my personal life. I find it sensitive, humane, wise, and entertaining.
I am also listening to an audio book by Svetlana Alexievich, Secondhand Time: The Last of the Soviets. I was born in the Former Soviet Union and left a few years after Perestroyka. I find this to be a fascinating chronicle about how everyday Russian citizens recount their past: what life was like during the fall of the Soviet Union and what it was like to live in the new, post-Soviet Russia.
If there was one takeaway or action point you hope people will get from your work, what would it be?
In the uncertain spaces of controversial diagnostic categories, such as ADHD, there is a need to respect and take into account mothers’ daily experiences and knowledge to create and maintain an inclusive environment for “troubled” children, on the one hand, and to challenge common cultural expectations from mothers, on the other.
The next few months we’ll be highlighting authors who have published in Culture, Medicine, and Psychiatry.
Tomás de la Rosa completed his doctorate in neuroscience at Federal University of São Paulo (Brazil) and is now a postdoctoral fellow at neuropsychopharmacology research group at the University of Cadiz (Spain). From his biological background, he also brings a particular interest in the philosophical and sociological dimensions of neuroscientific research, through the lens of critical and decolonial theory.
Neurodegenerative diseases are becoming more common as the global population ages, posing significant challenges for medicine. These diseases are progressive, long-lasting, and often lead to higher death rates. Research and medical practices are often influenced by power and politics, which can impact patient care. Drawing on ideas from philosophers Foucault and Mbembe, our article examines how aging, neurodegeneration, and death are managed. We argue that power dynamics shape the way knowledge about these diseases is produced, often overlooking the role of mortality. We also highlight the impact of colonialism on this knowledge, emphasizing its importance when considering death in these contexts.
Tell us a little bit about yourself and your research interests.
My primary training and research have focused on neuroscience and animal models of neuropsychiatric disorders. However, despite my background in basic biological and experimental research, I have been interested in the sociological and epistemological aspects of our laboratory practices since my PhD. It was during this time that I began to conceptualize a project exploring the politics of neurodegeneration.
What drew you to this project?
During my thesis in the neuroscience department at Universidade Federal de São Paulo, I studied cardiac and respiratory functions in an animal model of Parkinson’s Disease. The main goal was to explore the connection between neurodegenerative processes and these vital functions. This idea stemmed from epidemiological observations of increased sudden cardiac death in this population, an issue often neglected in neurological research. At that time, I began to familiarize myself with the work of Nikolas
Rose, who explores the politics of modern biotechnology. His work inspired me to investigate the formation of the discourse around neurodegeneration, from in vitro studies to clinical practice and broader societal implications.
What was one of the most interesting findings?
One of the most intriguing findings was the contrast between biopolitical and necropolitical deployments within biomedicine, highlighting different individuals and discourses. This phenomenon is not exclusive to neurodegenerative diseases or neurology. Through our study, we observed how some biopower mechanisms, designed to increase life expectancy, are developed within the same epistemological biomedical framework and spaces, such as hospitals, as necropower mechanisms aimed at erasing certain populations. In our view, this heterogeneous nature of power reflects the territorial and social organization and governance in liberal and colonial societies.
What are you reading, listening to, and/or watching right now?
I am currently immersed in Ana Maria Gonçalves “Um defeito de cor.” It offers a profound exploration of the Brazilian experience of slavery, told not through official historiography but through the perspective of an African woman searching for her long-lost son. This narrative exemplifies storytelling from the periphery, a theme we emphasize in the final section of our article.
If there was one takeaway or action point you hope people will get from your work, what would it be?
Recognizing how biomedical technologies are developed and articulated within a monolithic narrative of health and disease, that is necessarily incomplete and partial. A decolonial turn may help us decenter this narrative and include new ways of knowing and doing, accordingly to the multiple ways of being that exist.
The following article is part of the Culture, Medicine & Psychiatry March 2024 special issue, “Student Experiences of Covid-19 around the Globe: Insights from the Pandemic Journaling Project” which is guest edited by Heather M. Wurtz, Katherine A. Mason, and Sarah S. Willen.
This special issue explores how the Covid-19 pandemic has impacted the mental health and wellbeing of high school and college students in diverse locations around the world. The collection analyzes data collected by the Pandemic Journaling Project, a combined research study and online journaling platform that ran on a weekly basis from May 2020 through May 2022, and from complementary projects. Contributions draw on a range of data including PJP journal entries, semi-structured interviews with PJP participants, autobiographical writing by students, and conversations about engagement with PJP in classroom and community-based settings. This week we feature a brief blog post by the authors of “Cultivating Voice and Solidarity in Times of Crisis: Ethnographic Online Journaling as a Pedagogical Tool”.
This article is by: Sarah S. Willen, Associate Professor of Anthropology, University of Connecticut Kristina Baines, Associate Professor of Anthropology at the City University of New York (CUNY) Guttman Community College and affiliated faculty at the CUNY Graduate School of Public Health and Health Policy Michael C. Ennis-McMillan, Associate Professor of Anthropology at Skidmore College
Photo 1: Skidmore College students, isolated in quarantine, viewing campus activities from a window (2022).
In our piece, we discuss how online journaling – in general, and using the Pandemic Journaling Project (PJP) platform in particular – became useful for teachers and students at the height of the COVID-19 pandemic. Our essay synthesizes a series of conversations among three educators who specialize in medical anthropology: one of PJP’s co-founders and two anthropology faculty who taught with PJP in multiple classes at their respective institutions. We show how PJP gave students a chance to use ethnographic approaches to document their pandemic experiences – not just for themselves, but also as a forward-looking form of “archival activism.” At a time when participant-observation and other traditional teaching strategies had become impossible, PJP helped students learn from, connect with, and think critically and analytically about the pandemic experiences of people who were both similar to and also very different from them.
Tell us about how this project came to fruition.
After learning that both Kristina and Michael had begun teaching with PJP, Sarah brought the crew together for a sustained conversation that started with one-on-one conversations, followed by an online panel about the pedagogical value of online ethnographic journaling (at the 2021 Society for Applied Anthropology Annual Meetings) and eventually the three-way dialogue that became this co-authored essay.
What was one of the most interesting findings?
We were struck by the ways in which ethnographic journaling can help students appreciate what it means to bring your “whole self” to your ethnographic work – and how doing so can create new forms of data and insight, challenge mainstream misconceptions, help ease distress, and even – in some instance, have therapeutic benefit. Students documented a range of critical and creative pandemic responses that broaden understanding of a global health emergency.
Who might be interested in reading your piece?
We expect that anyone who lived through the first years of the COVID-19 pandemic, and especially people who were either students or educators (or both) during that time, will see aspects of their experience reflected in the piece. We hope that students who read it will come away with a better understanding of how much teachers scrambled to understand students’ experiences, connect with their students, and teach well under extraordinarily difficult circumstances. And we hope that educators who read the piece, especially those in anthropology and other qualitative social sciences, will see how online ethnographic journaling can serve as a valuable teaching and learning tool and that students’ voices offer valuable contributions to studies of pandemics.
If there was one takeaway or action point you hope people will get from this work, what would it be?
We recognize that lots of people don’t want to think about COVID anymore, or think about it right now. But when you are ready to think about it, we think our piece can offer useful insights on the value of online journaling in classroom settings. We also think it can help folks see the value of bringing PJP’s searchable Featured Entries page into your own teaching and learning experiences. In addition, our article will orient future scholars now that the PJP archive (housed at the Qualitative Data Repository) is open to external researchers.
The following article is part of the Culture, Medicine & Psychiatry March 2024 special issue, “Student Experiences of Covid-19 around the Globe: Insights from the Pandemic Journaling Project” which is guest edited by Heather M. Wurtz, Katherine A. Mason, and Sarah S. Willen.
This special issue explores how the Covid-19 pandemic has impacted the mental health and wellbeing of high school and college students in diverse locations around the world. The collection analyzes data collected by the Pandemic Journaling Project, a combined research study and online journaling platform that ran on a weekly basis from May 2020 through May 2022, and from complementary projects. Contributions draw on a range of data including PJP journal entries, semi-structured interviews with PJP participants, autobiographical writing by students, and conversations about engagement with PJP in classroom and community-based settings. This week we feature a brief blog post by the authors of “The Eschucha (Listen) Podcast Project: Psychosocial innovation for marginalized Mexican youth and young adults”.
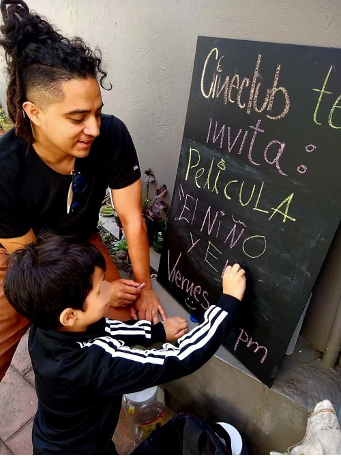
This article is by: Cristopher Bogart Márquez Rodríguez, Master’s student in Psychosocial Intervention, Department of Psychology, Catholic University of Colombia
The “Escucha” (Listen) Podcast Project” describes an innovative intervention project based in Mexico City, which sought to provide psychosocial support for young people in contexts of social exclusion. Youth participation in the project entailed weekly journaling with the Pandemic Journaling Project (PJP) — an online journaling platform and research study. Youth also engaged in weekly phone conversations with a member of the intervention team to give youth a space to express themselves and reflect on their lives and experiences. Regular and frequent communication with youth participants throughout the project helped foster a sense of trust towards the intervention practices and the intervention team. The project culminated in the creation of a podcast, in which each participant created a 2-5 minute chapter for the podcast about their experiences during the pandemic.
Tell us about how this project came to fruition.
Violence in Mexico has grown exponentially in recent years; one of the population sectors hardest hit by increasing violence is young people — especially those who live and coexist in contexts where violence is the daily norm. This sector is particularly vulnerable to different types of risks linked to material conditions and poverty. Despite increased need, there is a lack of emotional and therapeutic support programs that operate in marginalized communities. In my experience of around 13 years working with vulnerable groups, acting early can help prevent the reproduction of violent behavior. One of the objectives when intervening within these communities is to trigger cognitive processes that promote critical perspective of structural inequity, help youth reevaluate their abilities and potential, and strengthen their self-esteem. Bringing together the easy-to-use, digital platform of PJP with our own psychosocial tools allowed us to engage youth in these cognitive processes through dialogue, writing, and other creative outlets.
What was one of the most interesting findings?
One of our most interesting and important observations during the course of the project was the impact of the intervention on participants’ sense of wellbeing, as they described in both one-on-one conversations with team members, as well as in their journals. For young people who contend with overlapping forms of exclusion, it can be difficult to help them gain access to and engage in therapeutic spaces. But feeling truly listened to, for youth, can have a far-reaching effect. One of the project participants who had been incarcerated prior to the project and found the intervention particularly insightful, commented to an intervention team member: “If I had done something like this when I was younger, if someone had listened to me like this, with attention and without judging me, maybe my life would have been different.”
Who might be interested in reading your piece?
This article will be of interest to health professionals attracted by research and development of innovative, non-traditional projects aimed at young people in contexts of social exclusion.
If there was one takeaway or action point you hope people will get from this work, what would it be?
We can conclude by recognizing the impact of creatively-driven, contextually appropriate mental health interventions for youth. Socio-emotional work with young people in marginalized contexts in Mexico is not common, however, providing alternatives for support and professional accompaniment – as was done through this work – has made a notable difference in strengthening self-esteem among the youth participants.
The following article is part of the Culture, Medicine & Psychiatry March 2024 special issue, “Student Experiences of Covid-19 around the Globe: Insights from the Pandemic Journaling Project” which is guest edited by Heather M. Wurtz, Katherine A. Mason, and Sarah S. Willen.
This special issue explores how the Covid-19 pandemic has impacted the mental health and wellbeing of high school and college students in diverse locations around the world. The collection analyzes data collected by the Pandemic Journaling Project, a combined research study and online journaling platform that ran on a weekly basis from May 2020 through May 2022, and from complementary projects. Contributions draw on a range of data including PJP journal entries, semi-structured interviews with PJP participants, autobiographical writing by students, and conversations about engagement with PJP in classroom and community-based settings. This week we feature a brief blog post by the authors of “Seesaw Precarity: Journaling Anxious Hope on a Chinese University Campus During Covid-19”.
This article is by: Katherine A. Mason, Associate Professor of Anthropology, Brown University Jianmei Xie, Lecturer in Second Language Education, School of Foreign Languages, Guangdong Polytechnic Normal University
Photo 1: Photo from journal entry by study participant, April 14, 2022, Guangzhou, China
“Seesaw Precarity” is based on the Covid-19 experiences of a group of Chinese university students. We draw on journal entries that the students submitted to the Pandemic Journaling Project to argue that these students spent most of their undergraduate years living in a state of “seesaw precarity.” We define seesaw precarity as a long period during which many people in China were unable to predict from one day to the next whether they would be free to engage in the ordinary, everyday activities of everyday life. We trace student reactions and adaptations as they struggled to attend class, buy food, and see friends and family in the midst of unpredictable swings between openness and closedness. The seesaw nature of restrictions spurred anxiety among the students we followed, but also produced an optimistic mindset we refer to as “anxious hope.”
Tell us about how this project came to fruition.
This project resulted from a partnership between the co-authors that traces back to 2002, when we first met in Guangzhou, China to do a Chinese-English language exchange. We became friends and then colleagues and have kept in close touch over the years. We kept in touch during the pandemic, and we knew from our own correspondence that both professors and students were having really different experiences in China vs. the US. When Heather and Sarah and I (KAM) decided to put together a special issue on student experiences of the pandemic, I (KAM) thought immediately of reaching out to Jianmei (JX) to see if she’d be interested in writing something. She was, and we began meeting to put together the project that forms the basis for the paper. It’s been such great fun collaborating on this project and this article after so many years of more informal collaborations!
Photo 2: Photo from journal entry by study participant, April 10, 2022, Guangzhou, Chin
What was one of the most interesting findings?
I think both of us were pretty surprised at just how resilient the students we followed seemed to be during all of the crazy ups and downs of the pandemic in China. Jianmei had noticed and remarked on this before we even started the project, as she worked very closely with dozens of Chinese undergraduates during this time and frankly was amazed at how much better they seemed to be handling things than the adults in her life! We had talked about this before and then both observed it strongly in the data. The students were definitely struggling, and periodically did get upset, but they were really determinedly optimistic about the whole thing in ways that were quite inspiring.
Who might be interested in reading your piece?
I think our piece should be of interest to anyone who would like some deeper insights into lived experience during the pandemic in China. We get such a stilted, superficial view of people’s lives there through US media, and the focus is almost always on negative experiences and on resistance. Our article certainly doesn’t discount people’s negative experiences, but also provides a bit of a more well-rounded sense of the full lives people were leading, and how they managed to find joy in addition to the sorrow. We also provide some insight into why there was relatively little resistance to harsh control measures in China during the first two years of the pandemic.
If there was one takeaway or action point you hope people will get from this work, what would it be?
One big takeaway from this article is that people can handle an awful lot of uncertainty even over long periods of time, if they have faith in the system and are able to experience their chaotic situation as something that will make them stronger rather than break them. But this ability and willingness to weather a lot has limits. A lot of people started to hit their limit in China in late 2022, when the really strict control measures that they were living with started to work less and less well in controlling the virus, and the cycles between locking down and opening up became more frequent and more extreme.
The following article is part of the Culture, Medicine & Psychiatry March 2024 special issue, “Student Experiences of Covid-19 around the Globe: Insights from the Pandemic Journaling Project” which is guest edited by Heather M. Wurtz, Katherine A. Mason, and Sarah S. Willen.
This special issue explores how the Covid-19 pandemic has impacted the mental health and wellbeing of high school and college students in diverse locations around the world. The collection analyzes data collected by the Pandemic Journaling Project, a combined research study and online journaling platform that ran on a weekly basis from May 2020 through May 2022, and from complementary projects. Contributions draw on a range of data including PJP journal entries, semi-structured interviews with PJP participants, autobiographical writing by students, and conversations about engagement with PJP in classroom and community-based settings. This week we feature a brief blog post by the authors of “‘You would think she would hug me’: Micropractices of Care Between First-Generation College Students and Their Parents During Covid-19”
This article is by: Andrea Flores, Vartan Gregorian Assistant Professor of Education, Brown University Kate Mason, Associate Professor of Anthropology, Brown University
Photo 1: The first gen research team presents their work at the Society for Applied Anthropology annual conference in Santa Fe, New Mexico.
Our article is about first-generation college-going families’ attempts to care for each other’s mental well-being during the pandemic. We call these efforts “micropractices” of care, or the “little things” we do for each other like offering a drive, buying a small “treat,” listening, or offering a kind word. Sometimes these micropractices had the desired effect, and sometimes they did not. By closely examining these micropractices, we show how mental wellness is formed in the space between people in everyday, but critical ways.
Tell us about how this project came to fruition.
This project was a small pilot we conducted to see how parents and first-gen college students navigated the balance between the immediate challenges of the pandemic and long-term educational plans. Coming out of the pilot, we more closely examined how mental wellness in the present was tied to keeping the family aligned on shared future goals.
What was one of the most interesting findings?
Some of our most surprising findings from our longitudinal interviews two years after initial student journaling included the multiple ways that students adapted and thrived over the period of the pandemic and the benefits to university learning that many students identified that could be applied to improve access to higher education throughout Mexico. Numerous participants described the personal benefits of the adaptability of virtual learning that allowed for greater exploration of personal and professional projects while also allowing students to have greater flexibility with fulfilling their university coursework. Many participants emphasized the potential for virtual learning platforms to play a key role in overcoming social inequalities within access to higher education in Mexico. They identified that virtual platforms could potentially improve opportunities for some students to access a broader range of specialties and coursework, particularly for students living in rural parts of Mexico.
Who might be interested in reading your piece?
Our most interesting finding was the importance of matched expectations regarding a given micropractice. We found that when there was alignment and understanding between the motivations behind a caretaker’s efforts and the cared-for’s response, mental wellness was preserved. When there was disjuncture and misunderstanding, mental wellness was harmed.
If there was one takeaway or action point you hope people will get from this work, what would it be?
We hope that folks who work with first-gen students—as instructors, deans, counselors, physicians—would be interested in reading this piece, as well as first-gens themselves!
University staff who work with first-gens need to integrate understanding about the webs of relationships first-gens manage into their practice. Understanding students’ progress in school cannot be separated from their family ties.
The following article is part of the Culture, Medicine & Psychiatry March 2024 special issue, “Student Experiences of Covid-19 around the Globe: Insights from the Pandemic Journaling Project” which is guest edited by Heather M. Wurtz, Katherine A. Mason, and Sarah S. Willen.
This special issue explores how the Covid-19 pandemic has impacted the mental health and wellbeing of high school and college students in diverse locations around the world. The collection analyzes data collected by the Pandemic Journaling Project, a combined research study and online journaling platform that ran on a weekly basis from May 2020 through May 2022, and from complementary projects. Contributions draw on a range of data including PJP journal entries, semi-structured interviews with PJP participants, autobiographical writing by students, and conversations about engagement with PJP in classroom and community-based settings. This week we feature a brief blog post by the authors of “Thriving Despite the Odds: Digital Capital and Reimagined Life Projects Among Mexican College Students During COVID-19”.
This article is by: Heather M. Wurtz, Post-doctoral Research Fellow, Pandemic Journaling Project, University of Connecticut/Brown University. Maria Hernandez, MA, El Instituto: Institute of Latina/o, Caribbean, and Latin American Studies, University of Connecticut Madeline Baird, PhD Candidate, Department of Anthropology, University of Connecticut
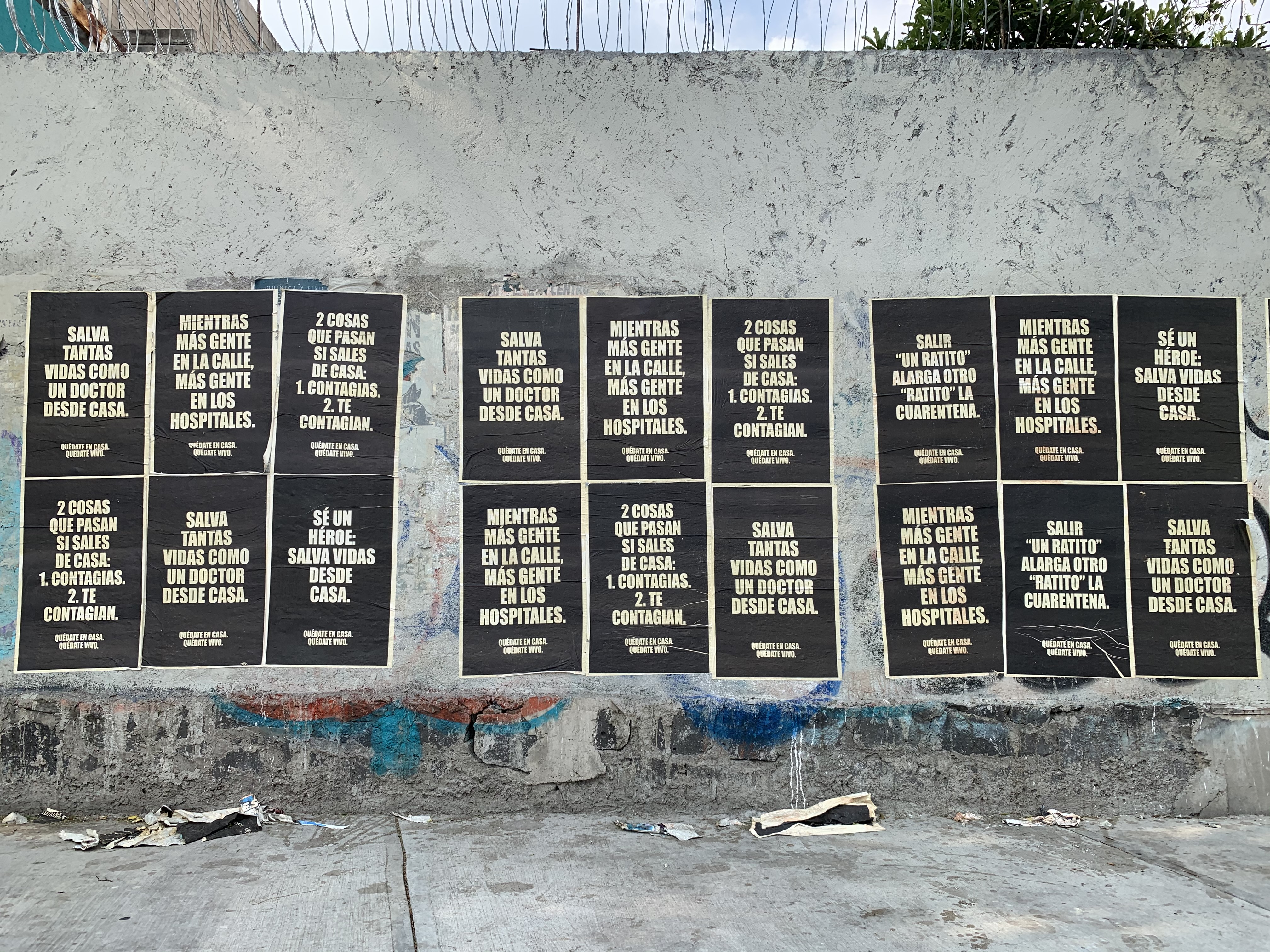
Photo 1: “Quédate en casa. Mayo de 2020” (Stay at home. May 2020) / José Antonio Cervera Jiménez / May 2020 – Mexico City. Photo from Picturing the Pandemic photo exhibition in Mexico City, MX.
Our article, “Thriving Despite the Odds,” examines ways that Mexican college students leveraged technology to cope with and overcome challenges related to prolonged school closures and other hardships during the pandemic. The study draws on in-depth interviews with and journals of 12 college students who participated in the Pandemic Journaling Project (PJP) – an online journaling platform and research study that chronicles everyday life during COVID-19. We found that by using technology to support their current and future endeavors, such as finding new ways to connect with others and to expand their professional skills, students experienced a renewed sense of purpose in their educational activities. For many, their engagement with technology also provided a source of coping with emotional distress, particularly in the way that it supported their ability to imagine a positive post-pandemic future – for both themselves and broader society.
Tell us about how this project came to fruition.
In the early months of the pandemic, nearly 50 college students from Mexico joined PJP and journaled periodically on the PJP platform for a time period spanning a few weeks to over 50 weeks, for some students. Their journals provided an important window onto the everyday experiences of students as they coped with the rapid transition to online learning along with a host of new challenges created by the pandemic, such as intensified caretaking roles and the illness and loss of loved ones. These insights raised compelling new questions for us about how students’ educational trajectories shifted or were reworked over time as a result of the pandemic and continuing hardships. All three of the authors have regional expertise in Latin America and recognized a unique opportunity for exploring changes in Mexican students’ lives and educational paths through follow-up interviews with PJP participants. The combined use of journals and interviews paints an illustrative picture of students’ experiences over the first two years of the pandemic, shedding light on the key role that technology played in students’ ability to adapt to and overcome adversity during a time of crisis.
Photo 2: “Staring at Doves” / Yolanda A. González G / April – June, 2020 – Mexico City. Photo from Picturing the Pandemic photo exhibition in Mexico City, MX.
What was one of the most interesting findings?
Some of our most surprising findings from our longitudinal interviews two years after initial student journaling included the multiple ways that students adapted and thrived over the period of the pandemic and the benefits to university learning that many students identified that could be applied to improve access to higher education throughout Mexico. Numerous participants described the personal benefits of the adaptability of virtual learning that allowed for greater exploration of personal and professional projects while also allowing students to have greater flexibility with fulfilling their university coursework. Many participants emphasized the potential for virtual learning platforms to play a key role in overcoming social inequalities within access to higher education in Mexico. They identified that virtual platforms could potentially improve opportunities for some students to access a broader range of specialties and coursework, particularly for students living in rural parts of Mexico.
Who might be interested in reading your piece?
Our article is written for anyone seeking to understand students’ experience during the global pandemic. Students worldwide experience a drastic shift from in-person to online learning. However, many students also found ways to cope and cultivate new ways of learning. Anyone reading this article will find that while many students struggled to adapt to online learning, some also found ways to develop and leverage their digital competencies for their future and to create a more equitable society. In addition, our educational leaders and policy readers may find these articles insightful in finding ways to promote and develop educational policies that support students’ online learning.
If there was one takeaway or action point you hope people will get from this work, what would it be?
For the students in our study, levering digital competencies and resources played an important role in their ability to maintain and adapt their life plans during a time of crisis. Their use of technology buffered their life plans not only in terms of expanding possibilities for future careers, but also for enriching their present lives – for example, by fostering their relations with others. These findings suggest that digital capital may promote college perseverance, especially in conditions that place constraints on in-person interaction. Digital competencies may also provide a source of coping with mental health distress by helping students cultivate a sense of human connection and belonging. While this is promising for some students, it also points to the potential role of technological disparities in intensifying social and health inequalities. These findings underscore the importance of closing digital divides, especially among marginalized communities already facing structural inequity.